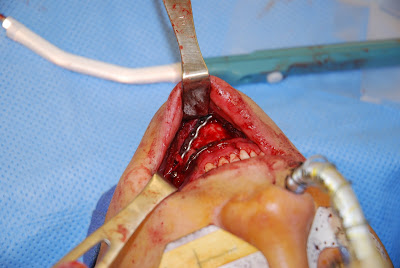
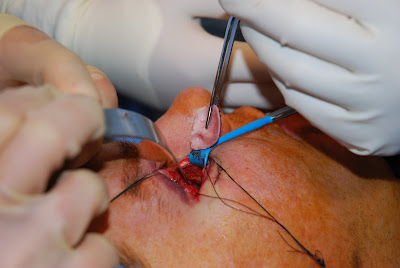
Mandible fractures are common and are some of the most enjoyable operations I perform. I prefer to treat many mandible fractures with open reduction and internal fixation, followed by a short course of intermaxillary fixation with Synthes, IMF screws.